
Building the bridge while crossing it: Rural healthcare in the Delta’s next era
 By Lora Delhom
By Lora Delhom
In January 2026, Mississippi’s rural health systems enter a new phase of federal health policy implementation. The One Big Beautiful Bill Act, passed in 2025, reflects a national effort to restructure health care spending and long-term sustainability.
For rural providers across the Mississippi Delta — many operating with limited margins and persistent workforce shortages — the focus is less on politics than on how new rules function in daily practice. Providers, administrators, and families are working to understand what the changes mean on the ground in a region already facing high rates of chronic disease, ongoing provider shortages, and the state’s highest infant mortality rate, which the Mississippi Department of Health has declared a public health emergency. As implementation begins, residents are navigating practical questions about coverage, cost, and access — not in theory, but in real life.
What Delta Residents Are Facing
To understand how these shifts are being experienced locally, The Leland Progress conducted a short community survey in December 2025 focused on insurance coverage, access to care, transportation, maternal health, and upcoming Medicaid work requirements.
While not statistically representative, the survey offers a snapshot of how policy assumptions intersect with lived experience. Respondents were, on average, more insured and economically stable than the Delta population as a whole: 73 percent reported employer-sponsored insurance, and only a small share were Medicaid recipients. Even so, more than half said they expected to lose insurance or were unsure about their coverage in the coming year.
On paper, access appeared strong. Most respondents reported reliable transportation, broadband access, and proximity to primary care. Yet nearly three-quarters said they had chosen to delay medical care in the past six months. Cost was the most frequently cited reason, followed by scheduling conflicts, childcare barriers, work constraints, and fear of unexpected bills.
The finding points to a central tension: in the Mississippi Delta, access does not reliably translate into care.
Administrative Whiplash in a Compartmentalized System
That disconnect is not unique to the area. Across the United States, health care delivery remains fragmented, with hospitals, clinics, and insurers operating on incompatible electronic medical record systems, billing platforms, and insurance verification processes.
In the Delta, however, fragmentation is intensified by geography, workforce shortages, and the absence of regional coordination. Most hospitals and clinics operate independently rather than as part of an integrated system, with patient records, billing practices, and coverage determinations varying widely between facilities — sometimes within the same county. Health policy experts often describe such arrangements as silos: individual structures standing side by side, but not meaningfully connected.
In this environment, policy complexity becomes administrative whiplash for patients. Routine care can feel financially risky when no one can clearly explain — before an appointment — whether a provider is in-network, whether a service is covered, or what a patient will ultimately owe. Errors in insurance filing, delayed claims processing, or mismatched coding can turn preventive care into months of billing disputes.
One insured Delta resident described seeking routine preventive care — a primary care visit and a mammogram — and later receiving a bill exceeding $1,800 after insurance was not properly billed. Repeated calls to the billing department went unanswered before the issue was resolved months later.
“It took nearly nine months to straighten out,” the patient said. “Now I’ve been putting off a recommended colonoscopy — not because I can’t get there, but because I don’t want to deal with the billing uncertainty again.” Another patient had to pay $800 up front for a colonoscopy at the time of service despite employer based coverage. They are now waiting for a refund.
National research consistently shows that administrative burden and cost-sharing confusion — rather than lack of clinics or transportation alone — are leading drivers of delayed care among insured populations, with disproportionate impacts on rural, low-income, and medically complex communities.¹
Specialists Are the Missing Link
Respondents most frequently cited difficulty accessing endocrinology, gastroenterology, rheumatology, dermatology and behavioral health — specialties closely tied to diabetes, autoimmune disease, gastrointestinal disorders, and other chronic conditions prevalent in the region. Many reported long wait times, out-of-region travel, referral complexity, and coordination challenges across hospital systems that do not communicate effectively.
Importantly, respondents did not frame specialist access as a transportation issue alone. Many reported the ability to travel if necessary. Instead, barriers centered on availability, lack of specialists in a day commute, cost uncertainty, and fragmented scheduling.
Taken together, the responses suggest that access to specialty care — rather than insurance status or clinic proximity — may be one of the most consequential pressure points in the Mississippi Delta’s health care landscape. National research has repeatedly found that rural communities face far greater barriers to specialty care than to primary care, driven by workforce shortages, referral bottlenecks, and fragmented delivery models.²
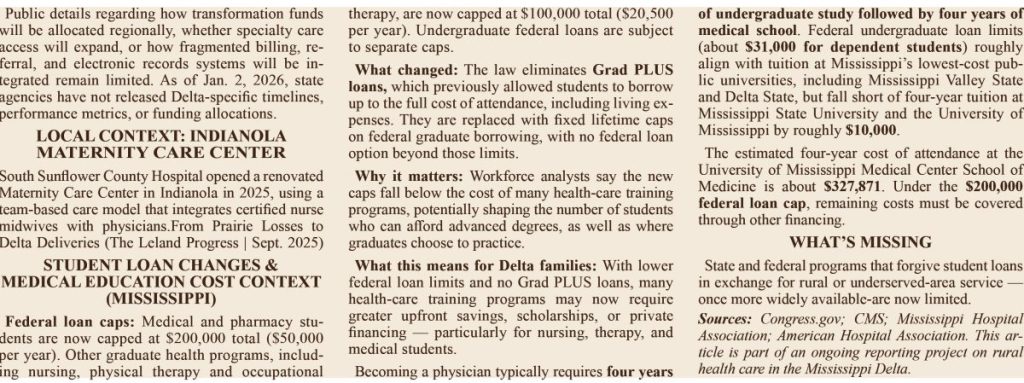
Workforce constraints extend beyond recruitment and retention. In a conversation for this article, a medical school administrator familiar with physician workforce planning said that access to specialty care is also shaped by national and state training pipelines. While Southern states continue to produce medical graduates, the administrator noted that the number of available residency positions — particularly in specialty fields — has not kept pace, creating bottlenecks that influence where physicians ultimately practice. Those pipeline constraints may be further shaped by new federal student loan limits, which workforce leaders say could affect who can afford advanced medical and health-care training and where graduates ultimately practice.
The administrator also described cultural pressures within medical training that can discourage students from pursuing flexible or dual-interest pathways, including guidance against ranking multiple residency types for fear of not matching. Over time, these structural and cultural dynamics narrow the pipeline into specialty care, particularly for rural regions that already face challenges attracting and retaining specialists.
Addressing specialty access in the Delta, the administrator said, will require not only local recruitment efforts but broader policy attention to residency capacity, specialty training pathways, and loan and housing incentives aligned with rural practice.
Federal Policy Assumptions Meet Delta Reality
The Medicaid work requirement embedded in the One Big Beautiful Bill intensifies these pressures. Under the law, most adults ages 19–64 must document employment, education, job training, or active job seeking to maintain insurance coverage.
While modeled after SNAP requirements, the standards are more difficult to meet in rural counties where work is seasonal, transportation is limited, and broadband access remains uneven. Although pregnant women, people with disabilities, and full-time caregivers are formally exempt, many Delta residents live in gray areas between those definitions — medically fragile but not officially disabled, or working short-term agricultural or contract jobs.
Federal policy increasingly assumes coordinated systems capable of tracking eligibility, employment verification, and billing across providers. In much of the Delta, those systems do not exist. The result is not theoretical inefficiency, but real instability: paperwork burdens, coverage lapses, and patient hesitation around seeking care amid uncertainty.
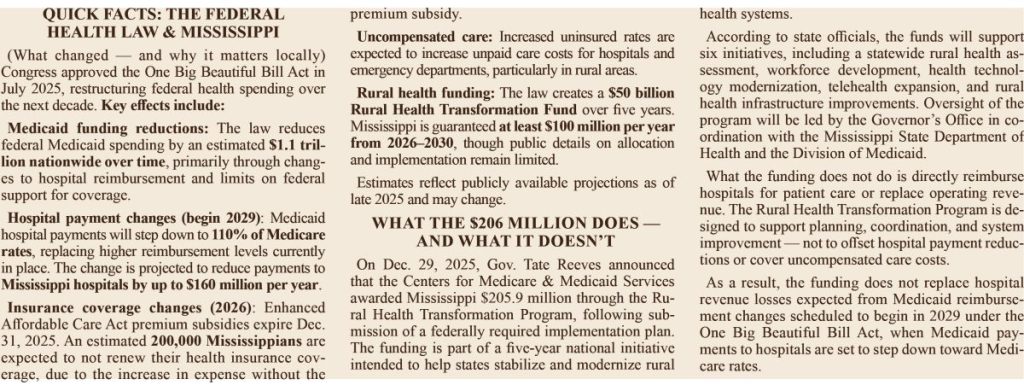
Key provisions of the federal law affecting Mississippi hospitals, insurance coverage, and the health-care workforce are summarized in the accompanying sidebar.

The Leland Medical Clinic at dusk, where new construction signals hope amid a shifting rural health care landscape.
The Delta Was Ahead of the Curve
Long before federal funding changes took effect, Delta leaders were already grappling with these structural weaknesses. In 2024 and 2025, regional stakeholders proposed frameworks aimed at building coordinated rural health systems, including shared specialty services, telehealth infrastructure, and regional referral networks.
A regional policy leader involved in Delta health planning said those efforts were intended to address fragmentation directly. “Those conversations were not about control,” the source said. “They were about coordination — keeping people in the Delta for care and bringing specialists here rather than forcing families to leave.”
None of the proposals advanced during the 2024 or 2025 legislative sessions ultimately passed. Public records and contemporaneous reporting indicate deliberations stalled amid unresolved questions about funding structures, governance, and the balance between regional coordination and local autonomy.
Among those efforts was the Mississippi Rural Regional Health Authority Act of 2025 (Senate Bill 2881), which proposed a coordinated regional framework but did not advance. During the same period, Mississippi submitted a Rural Health Transformation Program plan to access federal funds, though public details regarding its structure and implementation remain limited.
As a result, the next phase of federal health policy implementation will unfold in the Mississippi Delta without a coordinated regional rural health framework in place. It remains unclear what the state’s Rural Health Transformation Program under the One Big Beautiful Bill Act will provide through 2029, or whether elements of earlier discussions, proposals, or the 2025 Senate bill could advance in 2026.
Maternal Care and Trust
Survey responses related to maternal health were particularly notable. A majority of respondents indicated they would not choose to deliver at the new maternity center in Indianola, which opened in 2025. Respondents cited several factors influencing that decision, including skepticism about using the facility given its recent opening and resulting lack of long-term outcomes data, limited continuity of care following labor and delivery, and the absence of on-site advanced neonatal and emergency services.
Those concerns mirror broader qualitative reporting conducted for this article, including conversations with Delta women, families, and health care providers. Across those discussions, sources consistently emphasized the importance of established track records, continuity of care, and immediate access to higher-level specialty services when making delivery decisions. Several respondents said they would seek maternity care directly at larger regional hospitals, including facilities in Jackson and Memphis, rather than deliver locally, citing concerns about access to advanced care in the event of complications.
Neonatal intensive care and specialized emergency support are currently available only at larger regional centers such as Jackson and Memphis. Taken together, the findings indicate that while expanding local maternity services improves geographic access, it does not necessarily translate into patient confidence, which appears closely tied to demonstrated outcomes and proximity to advanced care.
Building the Bridge While Crossing It
The Delta is rebuilding its future while living its present. Clinics such as Leland Medical Clinic are expanding services even as federal funding tightens, while families navigate new rules within systems never designed to function as a whole.
For more than a century, the Delta has served as a proving ground — in agriculture, in public health, and now in health care policy. The question facing Mississippi is not whether reform is coming, but whether systems will be built to reflect the realities of rural communities whose economic, geographic, and workforce conditions differ sharply from those assumed in statewide policy design.
This is the bridge rural Mississippi is building while crossing it. The stakes are measured in delayed appointments, strained clinics, and whether families can remain rooted in the Delta — as well as whether new families can envision building their lives here.
Footnotes
¹ See, e.g., analyses by the Commonwealth Fund, Kaiser Family Foundation, and Congressional Budget Office on administrative burden, cost-sharing, and delayed care among insured populations, with documented disproportionate impacts in rural and low-income communities.
² See, e.g., Peterson et al., Health Affairs; Moy et al., Journal of Rural Health; O’Malley et al., Annals of Family Medicine; Andrilla et al., Journal of Rural Health; Chen et al., New England Journal of Medicine.
This coverage is supported by a grant from Press Forward Mississippi, part of a nationwide philanthropic effort to strengthen local news so communities stay informed, connected and engaged.




